The lifetime risk of dementia after age 55 years is 42%.
Basically a coin flip.
Source: Fang et al., Nature Medicine, 2025
I'm a psychiatrist, and almost every day someone sits across from me wanting to know what they can actually do about that number.
Sometimes it's the symptoms that brought them in. A word stuck on the tip of the tongue. Walking into a room and forgetting why. Losing the thread of a sentence halfway through.
Sometimes it's the opposite. No symptoms at all. But they watched dementia slowly take someone they loved, or a genetic test told them their risk runs higher than average. They don't want to wait until something feels wrong.
So I tell them the truth first.
There is no cure for dementia. Our very best treatments slow it by months, not years. And the changes underneath it begin years, sometimes decades, before the first symptom shows up.
By the time anyone feels different, a lot of the story has unfortunately already been written.
Then we'd get to work on the part they can actually control. Exercise. Diet. Sleep. Blood pressure. Hearing. The unglamorous things with real evidence behind them for supporting healthy brain aging.
And then, almost every time, the same question:
"What about supplements? Is there anything I can take to support my brain?"
When patients asked which supplement I'd recommend, I didn't have one.
I went looking for an answer. What I saw was worse than I expected.
- Products built around ingredients that have never been through a single controlled human trial.
- Formulas with 20+ ingredients at doses too low to do anything, claiming to fix brain health, gut health, immunity, and energy all at once, the supplement equivalent of promising everything and testing nothing.
- Products focused entirely on short-term effects: caffeine and stimulants that give you a jolt today while the long-term health of the brain goes completely unaddressed.
And it's not a niche problem. It's the whole category.
78%
of adults 40+ worry their brain is declining1
48%
of adults 50–64 already take a supplement for memory2
0
brain supplements endorsed by AARP's Global Council on Brain Health3
So I went looking for what actually held up.
I gave myself two rules.
First: I wouldn't take an ingredient seriously without randomized, placebo-controlled human trials behind it. The same bar I'd demand of any medication I prescribe.
Second: it had to target the long-term fundamentals of how a brain ages, not just a quick jolt of alertness that fades by dinnertime.
A small handful of ingredients cleared both.
What the research actually showed.
Low-Dose Lithium
A Brazilian research group followed patients for more than a decade and found that those who had received lithium showed slower cognitive and functional decline.4
A more recent study built on this and found that adults taking low-dose lithium showed about half the rate of verbal memory decline compared with placebo, one of the earliest changes seen in Alzheimer's disease and aging brains.5
But much of the lithium research had used lithium carbonate, the prescription form. At psychiatric doses, lithium carbonate carries real baggage: a narrow therapeutic window, drug interactions, and regular monitoring. That wasn't the long-term, practical answer I was looking for.6
So I looked at much lower exposures. In a 15-month randomized, placebo-controlled trial, Nunes and colleagues tested a microdose of lithium — 300 micrograms per day — and found that cognitive scores stayed near baseline in the lithium group while the placebo group continued to decline.7 A Danish nationwide study pointed in the same direction: higher lithium levels in drinking water were associated with lower dementia incidence.8
Then I looked at the form. A recent Harvard study suggested lithium orotate may be better suited for this purpose than lithium carbonate.9, 10
Vitamins B6 · B9 · B12
In a two-year trial at Oxford, a vitamin B6, B9, and B12 combination slowed the rate of brain shrinkage by about 30% versus placebo.11
A follow-up imaging analysis showed that the protection was concentrated in the very regions that tend to atrophy first with age.12
Lion's Mane
One study found that Lion's Mane helped preserve cognitive test performance, blood markers, and imaging measures.13
Another found that Lion's Mane improved cognitive testing scores, but those improvements reverted after participants stopped taking it.14
Magnesium Glycinate
In a placebo-controlled trial of older adults, magnesium glycinate improved cognitive measures over 12 weeks, with the analysis linking much of the benefit to changes at APOE-associated methylation sites.15
Clinical studies using magnesium L-threonate also found improvements in cognitive measures, suggesting the signal may extend across bioavailable magnesium forms rather than being limited to one version.16, 17
So we built the supplement we couldn't find.
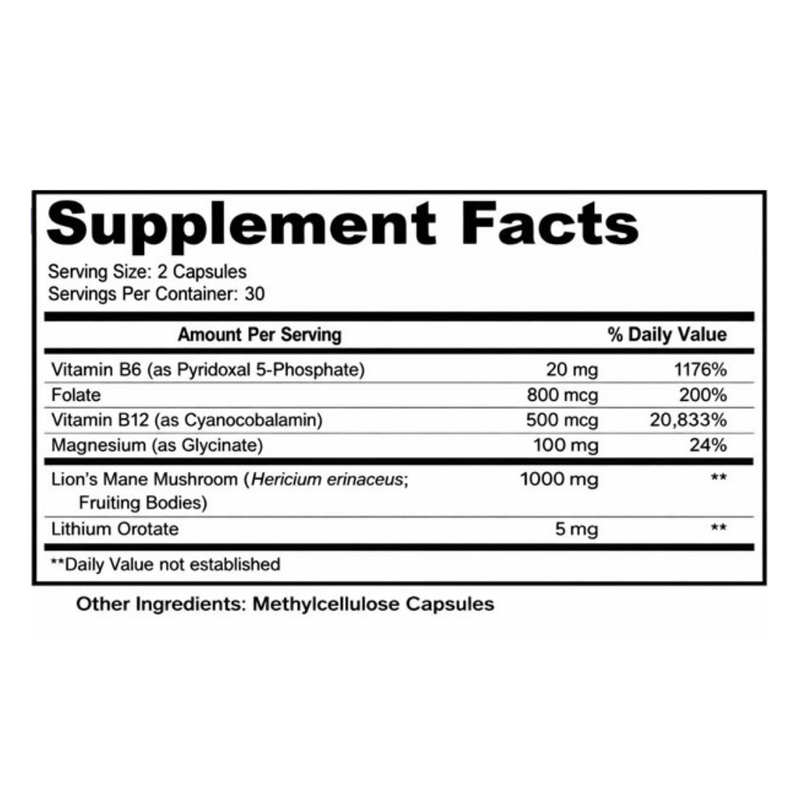
I brought in three other physicians to pressure-test every decision: the ingredient list, the doses, the form. We put these four ingredients together into one daily formula built around a single idea: support the fundamentals of how a brain ages, backed by evidence we'd actually stake our names on.*
We called it Mentaid. Four research-backed ingredients in two capsules a day. No proprietary blends. No filler ingredients. No stimulants.
It's the answer I wish I'd had every one of those times a patient looked at me and asked what they could take.
One thing to know: this is a long game, not a stimulant. The lithium trials that showed real benefit ran one to two years, whereas a trial only lasting 2.5 months did not show benefit.18 Don't expect a dramatic difference in week one. This is built for how your brain holds up over the months and years ahead.


Finally, something you can trust in the fight against brain aging.
Supporting over 1000 brains nationwide.
A doctor-formulated daily protocol designed for how your brain holds up over the months and years ahead.
Who Should Take Mentaid?
Anyone who's concerned about their aging brain and wants to do something about it while the still can.
Recommended Use
Take 2 capsules by mouth daily. No messy powders. No inconvenient gummies.
References
- AARP Research Insights: adults 40+ and brain-health concerns.
- University of Michigan National Poll on Healthy Aging: supplement use among adults 50–64.
- AARP Global Council on Brain Health report on supplements and brain health.
- Low-dose lithium trial with long-term cognitive and CSF tau follow-up. PubMed PMID: 36049127.
- Low-dose lithium trial reporting reduced verbal memory decline versus placebo. PubMed PMID: 41770546.
- Lithium carbonate clinical safety, monitoring, and therapeutic-window overview. NCBI Bookshelf.
- Nunes microdose lithium trial at 300 micrograms per day. PubMed PMID: 22746245.
- Danish drinking-water lithium population study and dementia incidence. PubMed PMID: 28832877.
- Harvard-associated lithium/orotate Alzheimer's disease research. PubMed PMID: 40770094.
- Harvard Medical School article on lithium and Alzheimer's disease research.
- VITACOG trial: B vitamins and brain atrophy. PubMed PMID: 20838622.
- Follow-up neuroimaging analysis of B vitamins and Alzheimer's-vulnerable brain regions. PubMed PMID: 23690582.
- Lion's Mane trial assessing cognitive, biomarker, and neuroimaging measures. PubMed PMID: 32581767.
- Lion's Mane placebo-controlled trial showing cognitive gains reversed after discontinuation. PubMed PMID: 18844328.
- Magnesium glycinate trial in older adults. PubMed PMID: 39009081.
- Magnesium L-threonate cognitive trial. PubMed PMID: 26519439.
- Magnesium L-threonate follow-up clinical study. PubMed PMID: 34111673.
- Short lithium trial that did not show benefit at ten weeks. PubMed PMID: 19573486.